For my own personal use only:
- Injection site sarcoma

Cat after radical surgery to remove injection-site sarcoma - Classic case: Mass at/near site of previous vaccination with vaccine up to ten years previously
- Dx: Follow the “3-2-1” rule created by the Vaccine-Associated Feline Sarcoma Task Force: Any mass that...
- Persists more than 3 mos after vaccination
- Is greater than 2 cm diameter
- Increases in size more than 1 mo post-injection
- Fine needle aspirate or incisional biopsy (often more diagnostic)
- Staging: histopathology, thoracic radiographs, CBC, serum chemistries, urinalysis, +/- CT and MRI
- Tx:
- Surgery at referral center - need radical excision; 5-cm wide margins, 2 fascial planes deep
- Adjuvant radiation therapy
- Adjuvant chemotherapy may benefit
- Pearls:
- Prognosis:
- Local recurrence/ invasion is most common cause of death
- Metastasis most common to lungs
- Median survival after surgery is 274 d at referral hospital vs. 66 d at primary care center
- Always document in medical record: vaccine name, serial number, expiration date, manufacturer, site and route of administration
- Individualize vaccine recommendations
- Association with specific vaccines or medications is controversial
- Vaccine site recommendations:
- Rabies: SQ distal right pelvic limb
- FeLV: SQ distal left pelvic limb
- FVRCP: SQ distal right thoracic limb
- Prognosis:
- Panleukopenia

Kittens are affected most severely by panleukopenia - Classic case:
- Dehydration, depression, fever, hypothermia, vomiting, diarrhea, seizures
- Thick intestinal loops
- Intention tremors; wide-based stance (cerebellar hypoplasia from in utero infection)
- Dx:
- Profound leukopenia (WBC count 500-3000/ul), thrombocytopenia, hypoalbuminemia
- Canine parvovirus fecal test
- May be accurate in cats 24-48 hrs post-infection (will be positive up to 2 wks post-FVRCP vaccine)
- Tx:
- Fluids: for dehydration and maintenance needs with IV, SQ, or intraosseous
- Plasma or whole blood if total protein less than 4 g/dl
- Parenteral B complex to prevent thiamine deficiency
- Antibiotics with gram-negative coverage (e.g., ampicillin)
- Treat persistent vomiting (metoclopramide, maropitant, odansetron)
- Pearls:
- Degree of neutropenia and thrombocytopenia parallel clinical disease and prognosis
- Use 1:32 bleach solution to kill parvovirus
- Vaccination is very effective prevention
- Classic case:
- Toxoplasmosis

Birds and rodents are intermediate hosts for Toxoplasma gondii - Classic case:
- Outdoor cat with access to rodents
- Indoor cats at risk from insects
- Clinical signs can occur mos to yrs after initial infection if immunosuppressed
- Chorioretinitis, neuro signs, GI signs, coughing, icterus, muscle pain
- Dx:
- IgM or IgG paired titers (4-fold increase 2-4 wks apart)
- Postitive IgG titer = previous exposure (yrs, even)
- IgM titer greater than 1:64 = active infection
- IgM or IgG paired titers (4-fold increase 2-4 wks apart)
- Tx:
- Clindamycin for 2-4 wks or 2 wks beyond resolution of clinical signs
- Corticosteroids are contraindicated
- Pearls: ZOONOTIC
- Can cause birth defects in a developing fetus if a mother is infected for the first time in her life while pregnant
- Simple prevention: "Pregnant women don't clean cat boxes!"
- Whoever does clean the box: do it at least once daily (oocysts sporulate and become infective in 24 hr) and wear gloves
- Dispose of cat feces in sealed bags taken to sanitary landfills, not in toilets or garden soil
- Keep cats indoors, prevent access to rodents and raw meat
- Prognosis: good with proper treatment
- Click here for more on human pregnancy and toxoplasmosis, courtesy of the U.S. Centers for Disease Control Toxoplasmosis page
- Classic case:
- Feline lower urinary tract disease
(FLUTD)
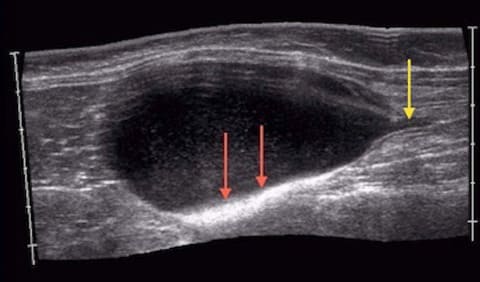
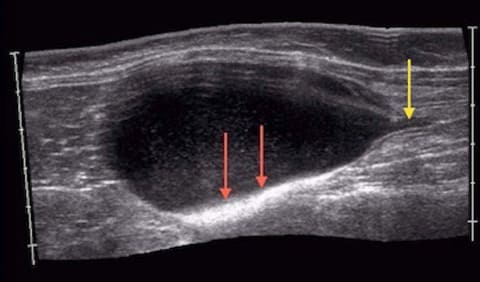
Obstructed male cat ultrasound. Dilated urethra (yellow arrow) and hyperechoic mineralized sediment in the urinary bladder (red arrows) - Classic case:
- Male, unable to urinate
- Straining in cat box
- Often obese
- Large, turgid bladder
- Hypothermia, comatose, bradycardia
- Dx:
- Urinalysis via catheterization: hematuria with leukocytes and crystalluria, analysis of urethral plug if present
- Azotemia, hyperkalemia
- Radiography: see uroliths
- ECG: tall-T-waves if hyperkalemia is severe
- Tx:
- Retrograde urohydropulsion
- Avoid cystocentesis and manual bladder expression
- IV fluids
- Treat bradycardia and/or tall, tented T-waves with 10% calcium gluconate as cardioprotectant
- Urinary catheterization with closed collection system
- Perineal urethrostomy is a salvage procedure when less aggressive management has failed
- Prevention: canned diet with extra moisture and weight management
- Pearls:
- Prognosis: 90-95% survival with prompt treatment
- Recurrence rate is 15-40%
- Antibiotics not warranted
- Classic case:
- Diabetes mellitus

Polydipsia is seen with diabetes mellitus - Classic case:
- Overweight or obese, middle aged or older, male neutered cat (or spayed female)
- May be very ill with diabetic ketoacidosis (DKA)
- Polydipsia/polyuria, polyphagia
- +/- Plantigrade stance due to diabetic neuropathy
- Dx:
- Fasting hyperglycemia (usually greater than 350 mg/dl)
- Urinalysis: glucosuria, +/- ketonuria, +/- active sediment
- Fructosamine: elevated with persistent (wks) of hyperglycemia
- Tx:
- Insulin twice daily (glargine or PZI are preferred for cats)
- Diet modification very important: canned, low carb (less than 7%)
- Do not use a high-fiber diet
- Pearls:
- Prognosis: good to excellent, remission possible
- Glucose curves should be done at home by client as in-clinic curves will be altered by stress
- Avoid repository glucocorticoids in cats as they can cause diabetes
- Classic case:




Images courtesy of WizardofOz (fibrosarcoma surgery), Dr. Uelsberg (kittens), Kalumet (ultrasound), Steve Jurvetson (polydipsia), Trish Steel (black cat), and Villa16 (cat and mouse).
Top Topic Category
Feline